
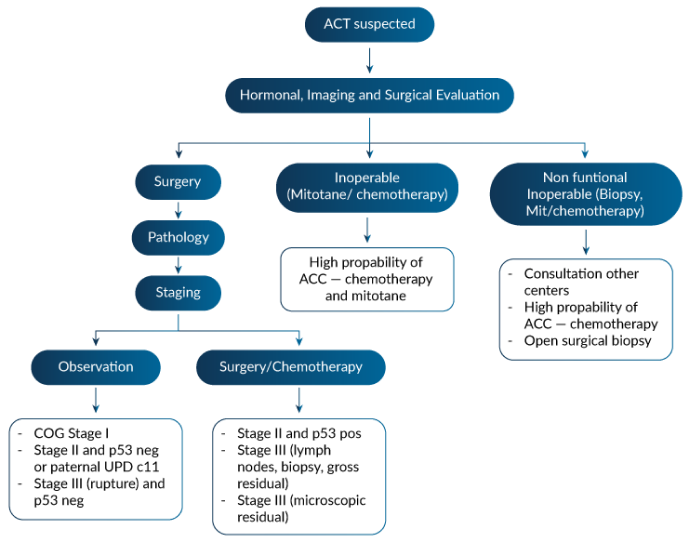
Summary of PACT Management
Goals
- To develop and implement a strategic support plan to find innovation, clarifying uncertainties surrounding size, genetics, histopathologic analysis and staging II classification;
- To improve metabolomics of mitotane (mitotane metabolites levels that may predict clinical outcome);
- The find the benefit of new anti-steroidogenic drugs: osilodrostat (Recordati) and the Orphagen new drug;
- To find new options for Immunotherapy, vaccine and CAR T
- Opportunities for surgery upfront:
- Surgery instead chemotherapy for children with microscopic residual disease;
- Neo-adjuvant chemotherapy in large tumors (anticipation of difficult resection, vascular extension);
- Role of surgery in recurrent and metastatic disease.
Raul Ribeiro compared the criteria and outcome of 3 different registries: (1) the French Registry, (2) the Italian Registry surgical protocols (including lymph nodes dissection) associated with adjuvant therapies and (3) ARARO332. We have to consider the large difference between very low germline TP53 mutations prevalence (<30% in Europe) and very high in Brazil (>90%) and age differences.
We envision a new proposition for stage II criteria to be initially launched at Boldrini Research Center under the coordination of Camila Daiggi
Summaries of three studies:
The French Group (Picard et al., Pediatric Blood Cancer, 2020)
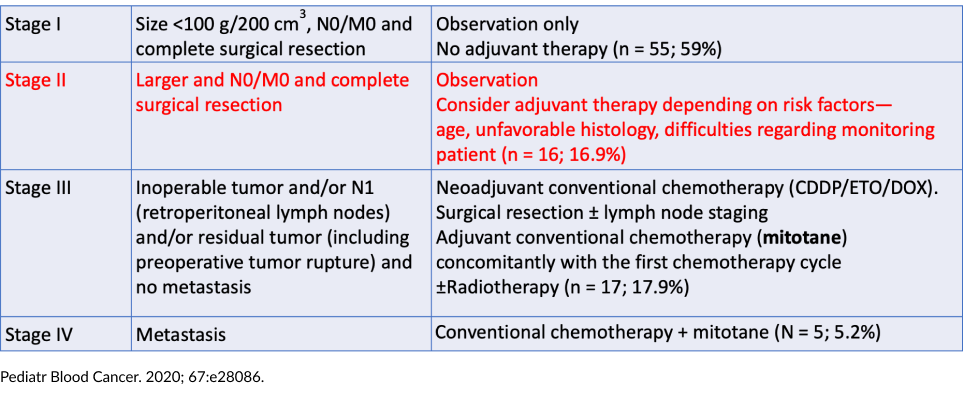
Outcome—Stage II disease (16 patients)
- 5-year OS of 93.3 and 5-year PFS of 78.8%
- One patient received adjuvant mitotane because of high tumor volume; it was stopped after 21 months due to neurological intolerance. The patient had a local relapse 4 years later and treated surgery (R0), and mitotane for a total of 8 years.
- Another patient developed lung metastasis after 4 months and subsequent liver metastasis after 15 months. The patient underwent complete surgical resection of metastases, combined with conventional chemotherapy and mitotane for 9 years.
- One patient died from an unrelated cause.
French cohort germline TP53 variants 22%
Expert Opinion—French Group
- Mitotane duration of treatment is unknown. Suggestion to use for 2 years, because the majority of relapses occur during this time.
- The objective role of mitotane is difficult to ascertain, and given the effect of other therapies, to extend its duration if it is well tolerated.
- The toxicity of mitotane is a major limitation. There is currently no evidence supporting the use of prolonged administration of mitotane.
- First-line systemic therapy consists of etoposide, doxorubicin, and cisplatin, in combination with mitotane.
- Second-line therapies have been used, with a very low impact on survival. The failure of second-line therapy should be considered palliative.
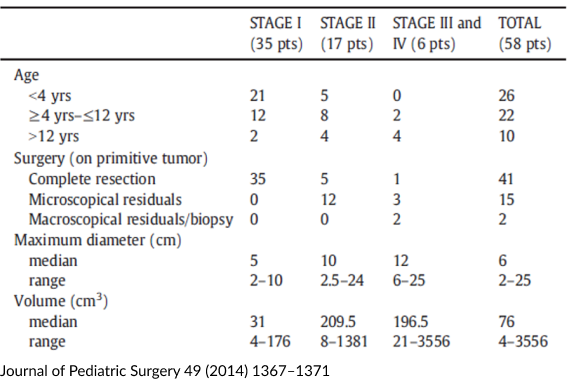
The Italian Group—Retrospective Analysis (Dall’Igna et al., Journal fo Pediatric Surgery, 2014)
- Patients < 19 years
- Stage I: Radical excision and tumor volume < 200 cm3 and subsequent normalization of hormonal blood levels
- Stage II: Radical excision, microscopic residual tumor, or tumor volume ≥ 200 cm3 and subsequent normalization of hormonal blood levels
- Stage III: Excision with macroscopic residual
- Stage IV: Metastases
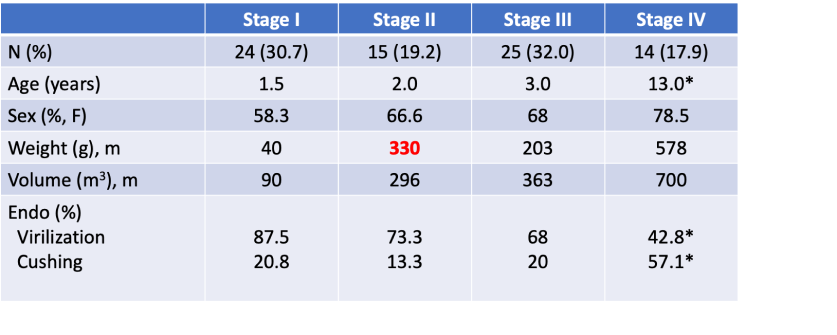
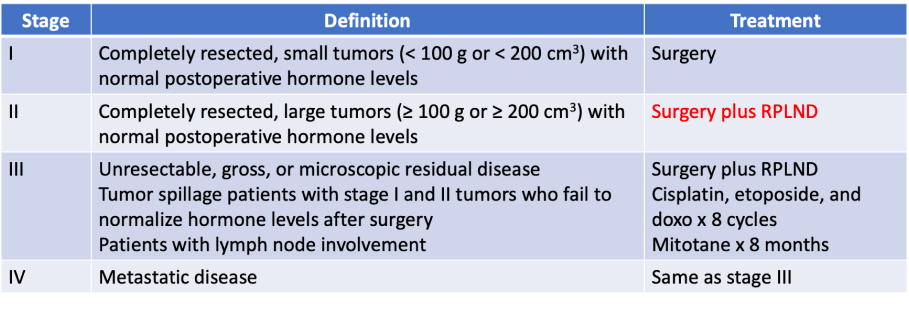
Children’s Oncology Group ARAR0332 Trial (Rodriguez-Galindo et al., J. Clinical Oncology)
- Prospective single-arm risk-stratified interventional study.
- Opened in September 2006 and closed in May 2013.
- Patients < 22 years, newly diagnosed, previously untreated adrenocortical carcinoma (central review, Weiss and Wieneke)
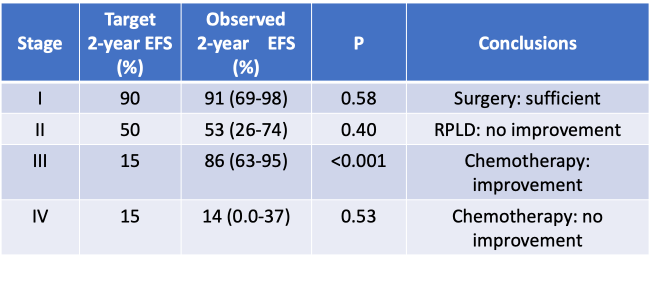
– Can RPLND improve outcome for patients with large (stage II) tumors?
– Can intensive chemotherapy (MTT/CED) improve outcome for patients with advanced (stage III and IV) disease?
IPACTR cohort germline TP53 variants 80%
Age, staging and clinical signs of ACT cases enrolled in ARAR0332
Treatment according to stage in ARA0332
Analysis of the Primary Results
Expert Opinions
- Surgery remains the mainstay treatment; the value of retroperitoneal lymph node dissection has not been defined.
- For patients with relapsed stage II and stage III, chemotherapy is associated with an improved outcome but is poorly tolerated.
- Innovative approaches are necessary for stage IV disease.
Stage I
- Five mitotane
- One radiotherapy
- One chemotherapy
Stage II (N total = 15)
- 13 mitotane
- Two chemotherapy
- Local radiation
Stage II Reevaluation
Possibilities to consider a score for Stage IIA and IIB (?)
The ICPACT project will evaluate a series of parameters and a new classificiation for Stage II.
Almost all Stage II ACT in Southern and Southeastern Brazil are germline TP53 (80 to 95%) and it is unclear the impact behind the low frequency of germline TP53 mutation in outcome of European pediatric patients

